

You may be forgiven for not knowing about apolipoprotein B – it is one of the lesser known cholesterol markers behind the likes of LDL, HDL and Total cholesterol. However, it has one of the strongest correlations with all cause mortality, slightly better than LDL cholesterol.
A raised apolipoprotein B indicates an increased risk of cardiovascular disease and death, noting that cardiovascular disease is responsible for around 25% of global deaths. The easiest way for people to measure their levels is with an apolipoproteins blood test.
What is apolipoprotein B
Apolipoprotein B, alongside LDL cholesterol, measures the presence of atherogenic particles in the blood that promote atherosclerosis. However, the two biomarkers don’t always reflect the same level of risk, and apolipoprotein B is a slightly better predictor of mortality.
In around 20% of the population, apolipoprotein B and LDL cholesterol will be discordant. This means that these two biomarkers may reach different conclusions about an individuals risk of heart disease. In some of these people, LDL cholesterol will underestimate their risk, and they won’t be aware of this until they test their apolipoprotein B.
How to measure apolipoprotein B
A standard lipid panel, like the ones a doctor might order, will usually not include apolipoproteins. Doctors will be fully aware of the research that suggests apolipoprotein B is superior [1], however a standard lipid panel is often chosen due to price.
Apolipoprotein B usually sits alongside apolipoprotein A as part of a more advanced lipid panel, which you may have to specifically ask your doctor for, or order via a private blood test.
An advanced lipid panel may cost £12-15 to process in the lab while basic lipids may only be £2-3. If you do purchase a private blood test, it makes sense to test it at the same time as other markers, like HbA1c for diabetes risk and CRP for inflammation.
Who shouldn’t measure apolipoprotein B
In the majority of cases there is no reason to avoid an apolipoprotein B blood test. Instead, there are certain populations where the interpretation of the result may be different.
Around 1 in 200 people have a genetic condition called Familial Hypercholesterolaemia, often abbreviated FH. The results of even a basic lipid panel will likely show very elevated LDL cholesterol, and the same will be true of apolipoprotein B. It’s important to note that up to 90% of people with FH aren’t aware they have it, and since lifestyle has a minimal effect it often results in lipid-lowering therapies like statins being prescribed.
Beyond that, advanced liver disease, severe kidney disease or very high triglycerides can distort particle estimates, and apolipoprotein B should be interpreted alongside other markers.
What do my results mean
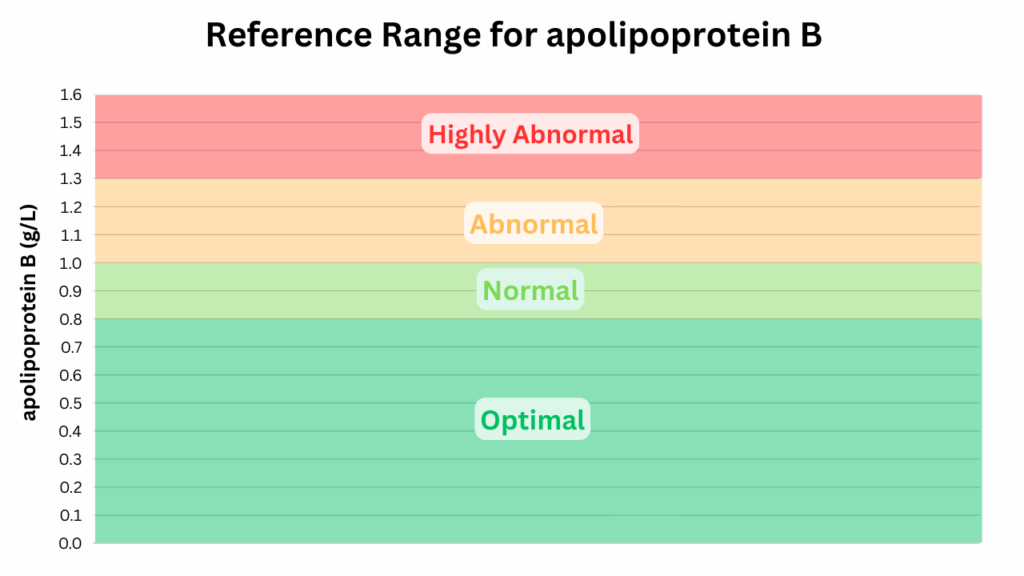
Here are a set of common reference ranges for interpreting your apolipoprotein B result:
- Optimal range: < 0.8 g/L (< 80 mg/dL)
- Normal range: 0.8 to 1.0 g/L (80 to 100 mg/dL)
- Abnormal range: 1.0 to 1.3 g/L (100 to 130 mg/dL)
- Highly abnormal range: 1.3+ g/L (130+ mg/dL)
The results from your chosen provider should come with a reference range that looks something like this.
Your apolipoprotein B results represents your average eating patterns and metabolic health over the previous few weeks of months, as well as any genetic component. Modifying your eating patterns to reduce saturated fat and increase fibre may be visible in blood markers in as little as 3 to 4 weeks*.
*As stated earlier, those with FH will often struggle to bring their result in to the normal range, and may require lipid-lowering therapy
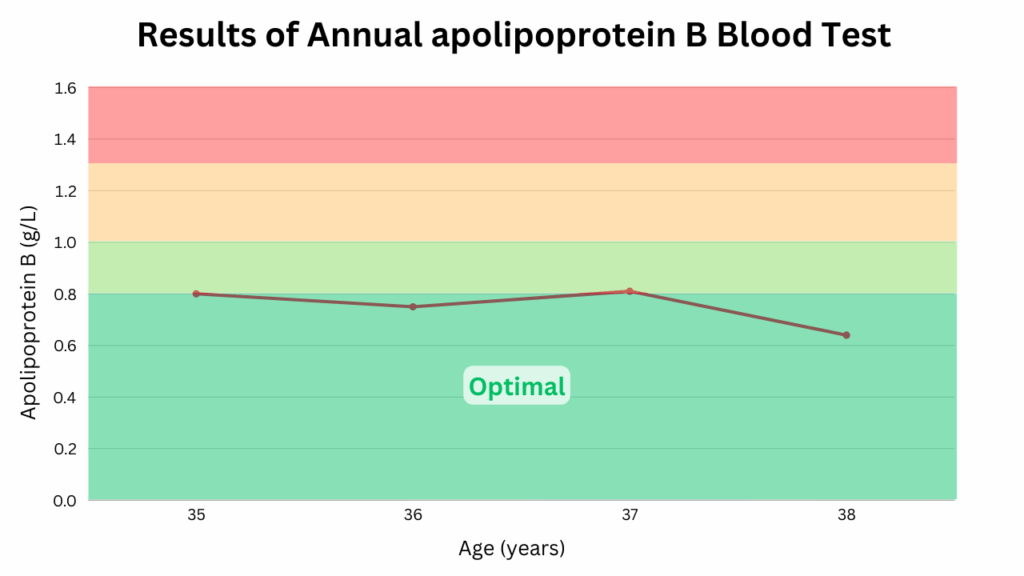
Tracking apolipoprotein B over time
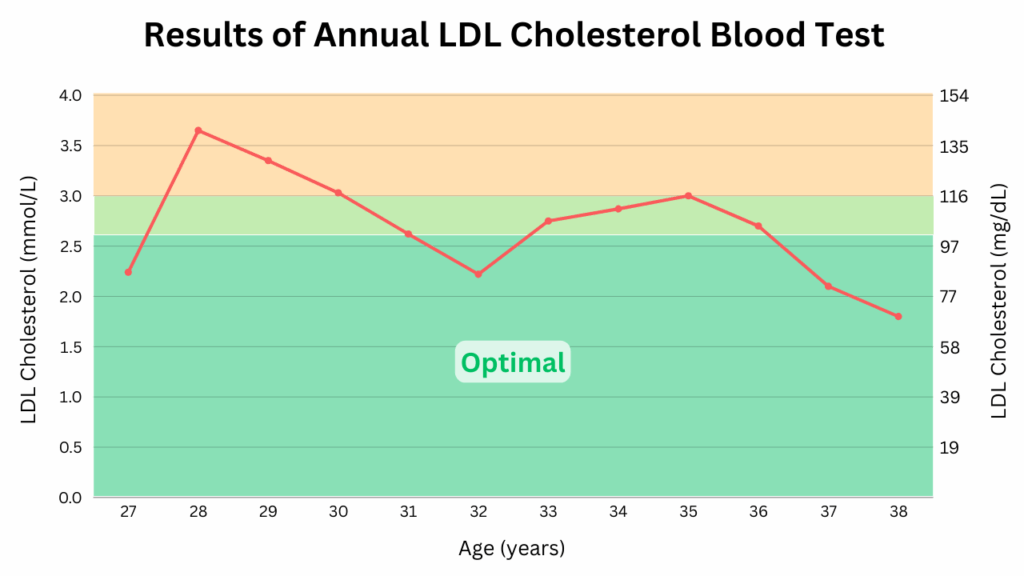
The test is worth repeating every 3 to 6 months, particularly if you sit outside the normal range. I have been tracking my LDL cholesterol since 2014 and my apolipoprotein B since 2022.
While apolipoprotein B is the superior marker, practically speaking it’s still valuable to measure your LDL cholesterol over time. In the majority of the population the LDL cholesterol result will convey the same level of risk as the more expensive apolipoprotein B test.
There are two lifestyle changes I have found to reliably reduce both my LDL cholesterol and apolipoprotein B:
- Reducing saturated fat
- Increasing fibre
I’ve personally found the ratio of these in the 21 days prior to a blood test to be very predictive of my LDL cholesterol result. My result of 3.0 mmol/L at the age of 35 was the result of a roughly equal ratio of saturated fat (30 grams) and fibre (30 grams) per day.
By age 38 I had lowered my LDL cholesterol to 1.8 mmol/L by reducing saturated fats to 18 grams/day and increasing fibre to 55 grams/day. Therefore my ratio of saturated fat to fibre moved from 1.0 to around 0.33.
[1] Apolipoprotein B compared with low-density lipoprotein cholesterol in the atherosclerotic cardiovascular diseases risk assessment, F.Galimberti, M.Casula, E.Olmastroni 2023